We’ve come so far in ketamine treatment for depression, and we still have so far to go.
KRIYA held the first conference on ketamine treatment for depression in 2015. Now, 5 years later, there are several medical conferences that support the exchange of information in this field. Raquel Bennett, the founder of KRIYA – The Ketamine Research Institute – says that ketamine is a flexible tool and should be used with freedom and skill. She urges clinicians to make the most of the flexibility of ketamine.
This is the last conference by KRIYA that will be held in this format, according to Dr. Bennett. She plans to possibly shift to an online format next year to accommodate the huge numbers of clinicians who wish to be included.
What’s more, KRIYA has supported, from the beginning, the use of ketamine by different routes and for varied conditions, and encourages participation from providers across the gamut of ketamine applications. So we’re a wonderfully diverse crew who come together for these conferences. As for me, I know that I’ve learned so many things and forged new friendships and collaborations from KRIYA conferences.
And…my own contributions have been so warmly received. As far as the educational gathering, there are psychiatrists, psychologists, therapists, ER physicians, pharmacists, anesthesiologists, neuroscientists, nurses, and experts in consciousness medicine.
Raquel Bennet, Psy.D. Stepped Up as a Leader in the Field of Ketamine for Depression
Dr. Bennett reminds us she has created a “tasting menu,” if you will… from
all corners of the field. At this conference, she opted for breadth vs depth to make us privy to all that’s happening in the field of working with ketamine. And she emphasizes that speakers are working from different paradigms. So, she urges us to listen for the paradigm they report from….and learn.
And she’s right when she says that ketamine is a flexible tool that contributes to a variety of needs. When a patient is too depressed to talk, ketamine lightens depression so they can participate in talk therapy. To help manage severe pain and the depression that goes with it. It can help the patient go deeper into therapy, and explore their traumatic experiences gently. It can treat acute suicidal thoughts and prevent hospitalization. And she says, it can induce mystical visions for existential exploration.
Raquel had much, much more to say, but I want to mention some of the other speakers.
Brent Turnipseed, MD and Lindsey Slater, LPC, from Austin, TX talked about their use of EMDR in ketamine-assisted therapy.

In PTSD, the body’s own reaction to a patient’s traumatic memories activates adrenaline , which prevents their ability to process their trauma. Ketamine can calm the body enough that they can process the trauma without the distraction of adrenaline. As a result, it can help relieve their fears.
EMDR works by helping the patient desensitize by brief exposures to the trauma, then by redirecting the patient’s attention, EMDR induces a relaxed neurological state similar to rapid eye movement (REM).
Elias Dakwar, M.D., psychiatrist and the addiction researcher we’ve often talked about before, gave a wonderful presentation.

He presented a thought -provoking talk on meditation and mindfulness as it relates to ketamine in treating addiction.
The field of ketamine for psychiatric disorders, including addiction treatment, continues to wrangle with how to take ketamine into psychiatry but that’s because our paradigms are problematic. Mainstream psychiatry has tried to cut ketamine down to size instead of using this extraordinary medicine as a DISRUPTOR.
Dr. Dakwar entered addiction research after a long time practice of meditation and with great compassion for the patients he sees.
He described his previous and current work in detail–look for it in the journals.
Ian Mitchell, M.D., Emergency Medicine in British Columbia,
spoke about the uses for ketamine in the emergency department. He spoke about its use for sedation during an emergency procedure, such as setting bones, repairing wounds, or the removal of foreign bodies, pediatric sedation for the same types of procedures, sub-dissociative dosing for pain management, especially for neuropathic pain, to prepare a patient for intubation, sedation for the out of control, prehospital pain relief, and to manage an overstimulated patient.
In British Columbia, ambulances are equipped with intranasal ketamine for prehospital pain management as a result of the PAIN-K trial. More of ketamine’s flexibility.
Wesley Ryan, M.D., psychiatrist from Marina del Ray, CA, Parria Zarrinnegar, M.D., psychiatrist in Portland, OR, and Daniel Barton, M.D., psychiatrist from Nashville, TN all presented riveting case reports.
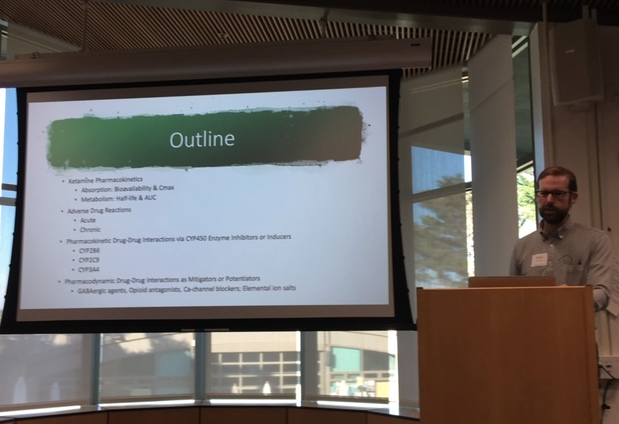
Kelan Thomas, Pharm.D,
spoke about adverse reactions and drug-to-drug interactions that have been documented with ketamine. So important and so well-done.
Annie Oak, a journalist from the Bay area, spoke on the use of ketamine outside the medical setting.
Gita Vaid, M.D., psychiatrist and psychoanalyst, spoke on using ketamine in psychoanalytic psychotherapy in very long session. She talked about how she has witnessed ketamine help patients relax and defenses soften so they can have freedom to talk. The psychotherapist builds relationship with the patient and it can be transformational.

Jason Wallach, Ph.D., is a pharmacologist and neuroscience researcher whose energy and depth of knowledge captivates us every time he speaks. He spoke about the neuroscience and pharmacology of ketamine. Gave an update on some of the other dissociative drugs he’s tested. (I think he’s tested them all!) He made the point that ketamine has been called a dirty drug because of the receptors it hits ex-vivo and in animal models — but that’s not true. It’s really one of the more selective drugs of this class at the doses used in people.

Jessica Katzman, Ph.D., and Harvey Schwartz, Ph.D., spoke about bumps in the road they’ve discovered with ketamine assisted psychotherapy and in the integration work that follows treatment… What is integration? It comes from a latin word that means “to make whole” or “to begin again.” Bring your clinical compass, but don’t forget your humanity. A beautiful duo talk with lots of clinical examples.

Eli Kolp, M.D., a pioneer in ketamine treatment, gave a beautiful talk on the phenomenology of ketamine-induced dissociative states.
There were so many other speakers and so much to absorb–my computer battery kept dying down, so between Surface notes, handwritten notes, and photos, I can’t do justice to the breadth of expertise in the room, and the excitement.
Greg Wells, Ph.D. Sylver Quevedo, M.D., Veronika Gold, M.F.T., Eric Sienknecht, Psy.D. presented as a panel on their model of coordination of care between prescriber and psychotherapist. Peter Koshland, Pharm.D. talked about how to work with a compounding pharmacy for varied compounded preparations of racemic ketamine. Nate Schmidt, A.R.N.P spoke about scheduling and billing logistics.
Sunday was a treasure with a very special presentation by Francoise Bourzat on the Use of Sacred Medicines in the Age of Technology and Medicalization. It was a delight to meet her. She captivated the audience, and her new book, Consciousness Medicine, is a wonderful synthesis of her life’s work.
Kelley O’Donnell, M.D. and Christian Yavorsky, Ph.D. are doing yeoman’s work with KRIYA and presented an excellent (and not dry!) talk on Measuring Clinical Outcomes: Scales and Assessment Tools. And in addition to the training for Ketamine Assisted Psychotherapy that Raquel Bennett presented and discussed earlier in the conference, Jennifer Dore, MD presented a model of training for Ketamine Assisted Psychotherapy developed by Phil Wolfson, MD and Julane Andrews, that they have used around the country.
IV Ketamine can STOP suicidal thoughts fast…Now that’s flexibility of ketamine!
On the last day, and as the next to the last speaker, I took the podium to share my data in working with patients in my own practice, and showing how IV ketamine infusions can stop suicidal thinking, and save patients from having to go to the ER or be hospitalized.

With heartfelt gratitude. These are my people–the clinicians and many of the greats in the field (who were in the audience) who launched my interest, encouraged my work, supported my writing–and showed me how to apply for an IRB. It’s amazing how much can happen in a year. So I saved the newest data and my newest results (using a new protocol and a new rating scale) for my colleagues and my friends here at KRIYA. I wanted them to hear it first.
I wanted to give back to those who have sparked my imagination, nurtured my interests, given wind to my sails.
It gives me such joy to share how this remarkable medicine that can do so much, can also save a life in a short time. And to see clinicians in practice eager to take this information home.
And that’s the beauty of meeting together at KRIYA and swapping stories and describing outcomes and victories that have restored the lives of people we work with.
Looking Back…and Reaching Forward – Preserving the Flexibility of Ketamine
It’s been such a busy fall with travel and speaking engagements each month… along with treating patients. (I’m sure my colleagues are as tired as I am. We need a vacation. Seriously.) But it’s gratifying to look back and know all this information that’s been shared will improve the lives of people we each cross paths with after KRIYA and all the other conferences.
I know these reports “from the front” can seem science-y and vague, but I want you to see how hard clinicians, neuroscientists, and practitioners of all types are constantly working to learn the breadth and depth of what ketamine can do to help people live better, improved lives. That’s really what it’s about. Ketamine’s flexibility allows for treatment that can turn your life around.
And if you’ve been reading along, and wondering if there is help for you, call us. In spite of all the travel and bustle, we’re still in all this to help you get better, live better, and have the ability to build a truly fulfilling life.
You owe it to yourself to try, if you’ve not found a medicine that works for you. It’s not that ketamine is a cure-all for everyone, but it works in so many areas of your brain, that it can restore areas damaged by stress and trauma in most people who are treated with it.
As the holidays approach, give yourself the best chance you can to enjoy the time ahead and the new year that follows.

To the restoration of your best self,